Did the Government abandon a working strategy when it shut down contact tracing after the now notorious March 12th COBRA meeting that decided to move from the “Contain” to the “Delay” phase of its flu-based pandemic plan? It’s what I said at the very beginning of April:
the worrying thing is I think we might have had a working strategy and abandoned it out of panic
— Alex Harrowell (@yorksranter) April 1, 2020
Self-publicity aside, it’s perhaps the most important question in any discussion of this disaster. This Grauniad piece contains a startling data point:
Public Health England, overseeing the scheme, believes compliance will be good, pointing out that it was able to trace and isolate 95% of contacts of cases before testing and tracing was abandoned on 12 March.
The celebrated Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts paper, which modelled the impact of different levels of contact-tracing effectiveness on simulated epidemics characterised by different values for parameters such as R0 (average transmissions per case) and k (overdispersion, or clustering), appeared in The Lancet on March 5th but had been available in preprint since mid-February. The following chart illustrates the key finding.
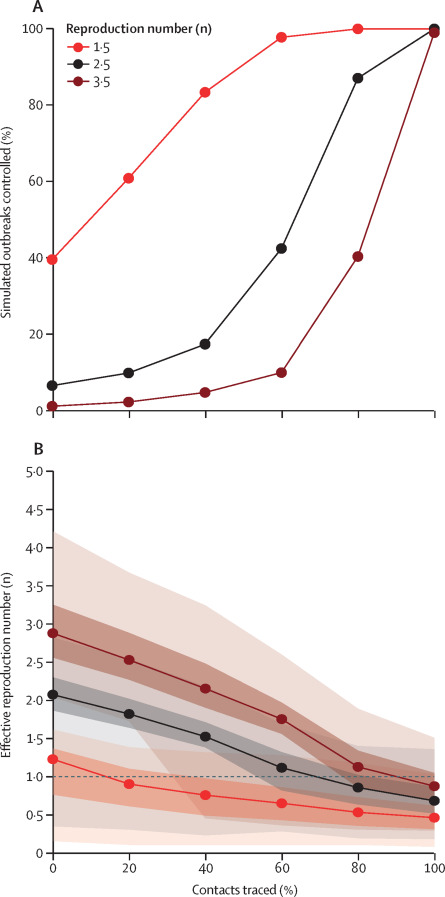
If 95% tracing really was achieved, even an outbreak with an initial R0 of 3.5 might have been contained. (Here’s another more recent paper with similar conclusions.) Current estimates of the real value put it much lower, between 2 and 2.5 for the Diamond Princess cruise ship outbreak, with a very high proportion of transmission coming from super-spreading events. If the PHE source speaking to the Guardian actually means 95%, in the sense of the number, 95 out of 100, rather than a general impression that compliance was good, this would also explain why the UK case numbers remained stable pretty much up to the Thursday when everything fell apart.
Interestingly, there is data that tends to corroborate an extraordinarily high degree of public consent and cooperation in the early stages of the crisis. Apple’s monitoring of requests for directions through Apple Maps suggests that most of the decline in mobility in the UK happened voluntarily, before the official lockdown on the 23rd of March:
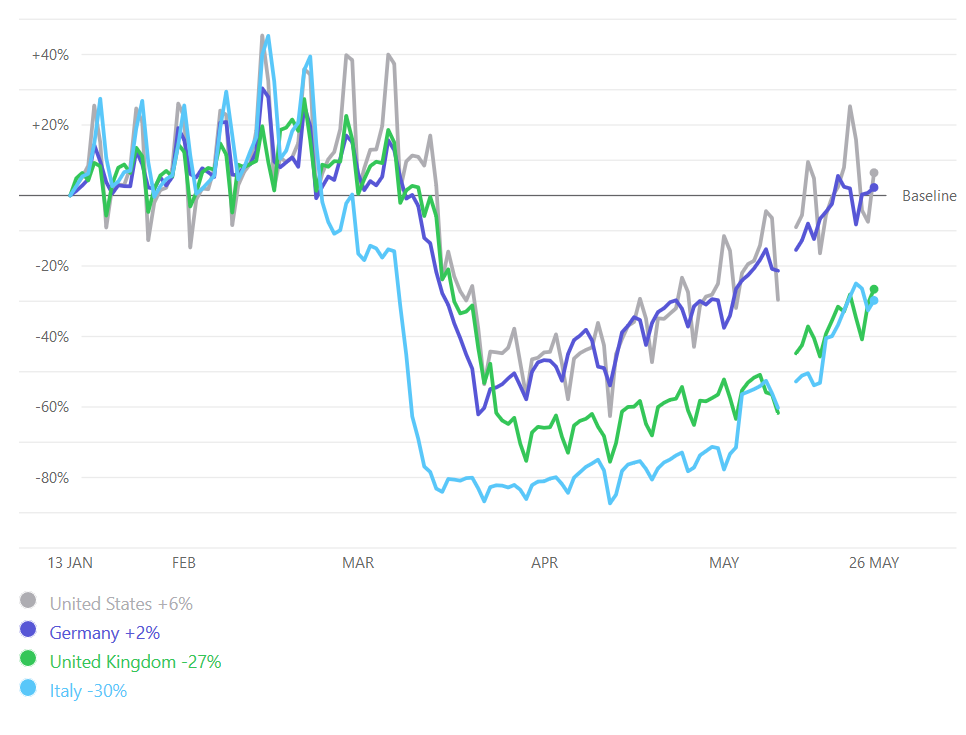
This implies the Government has perpetrated an appalling disaster out of panic and an apparent inability to take details like managing a call centre seriously. The big question is whether the public spirit demonstrated in March and April can now be recaptured, after, well, this.
I mean it with the call centre,by the way. Much media reporting at the time had “Whitehall sources” complaining about NHS 111, which was a key element of the test-at-home protocol. However only Kate Osamor MP seems to have taken this up as a political issue, because if we started caring about call centres, where would it end? This is likely to become a political issue again very soon so you may as well skate to where the puck will be.
As the author of The Churchill Factor didn’t say: We will fight them on the beaches. We will fight them on the landing grounds. And then we will make a hash of the admin, give up, soil ourselves with fear, throw our rifle behind a hedge, and scarper, leaving everyone else to their fate. After all, what’s in it for me?
And it is Johnson who’s the problem. There was a reason the Government abruptly switched from a communications strategy implementing the Krebs principles to one that emphasised a rolling cast of ministers, about the same time things got serious. I contend that No.10 decided to “get a grip” and drove the clown car off the cliff.
(Not that Shadow Health Secretary Jonathan Ashworth MP helped much by demanding in Parliament that the Government move to the delay phase. If he didn’t know the delay phase meant no more tracing, he should have done.)
Update: This new paper uses genetic sequencing to determine if very early cases in Germany and Washington State were actually related to later outbreaks, and found that they were not, and therefore, that the initial public health response was successful.
Panic is certainly a feasible explanation given what we know about the character of Johnson and those in his Government. Although panic over what remains a moot point.
Because a range of other known characteristics such as arrogance borne of a lifetimes background of class privilege about always being right and stubbornness about not changing decided policy also have to be considered. Not to mention the 100% record of estrangement from the truth and lying through his/their teeth every time they open their mouths.
The communicated and projected wisdom is that the “panic” which generated a supposed change of tack from the culling the ‘economically inactive’ herd approach was down to “The Science”. And if anyone believes a single word uttered by these charlatans on anything I have a second hand bridge for sale.
The Imperial College Report was publicly issued on Monday 16 March, the day of Johnson’s first TV address to the nation (you know, the Churchillian one in which he politely asked private industry, if its not too much trouble, if they could possibly see their way to switching a bit of production to ventilators – as though Churchill would have taken the same sanguine and grovelling approach with spitfire production). Yet it took five days of dither and drift until Friday 20 March for Johnson’s Government to make a decision to publicly announce an official “lockdown.”
If that was panic it was certainly in slow-mo mode.
Yet, coincidentally, this was a decision taken shortly after his widely publicised phone call with Macron – see here for example: https://www.telegraph.co.uk/politics/2020/03/22/emmanuel-macron-threatened-close-uk-border-unless-pm-clamped/
In which the French threatened to close their borders to the British if Johnson didn’t get his finger out. A threat which would not just have closed the French ports to tourists but also to trade, threatening vital UK supply chains. In such an eventuality its reasonable to anticipate the Dutch would have followed suit. With Rotterdam being the deep water port through which the vast majority of UK global supply chains are dependent it is this, rather than “The Science” which is more likely to have caused sufficient immediate panic to announce apparent changes to the herd immunity policy later that same day. No one takes five days to panic.
“Apparent” because to be effective a lockdown – as currently popularly defined and touted – has to have competent, coherent and practical support systems in place to make it work properly in terms of the expounded rationale. In this instance “The Science.”
Johnson and his Government had to be dragged kicking and screaming to that apparent about face. Ports of entry were and still are allowing unfettered travel into the UK and onwards with no containment and tracing protocols. I remain amazed at arriving back in Heathrow from India on March 2 with a tour party consisting of the older demographic the majority of whom were dosed up to the gunnels as a result of cold like symptoms of fever and chesty coughs to find no checks or containment protocols in place at UK ports of entry. To be honest there was concern that we might not get back into the country – which I have to concede was a tad optimistic given the track record of the fat owl of the fourth form Eton Remove and his cronies.
That in itself is important as the most comprehensive real data (as compared to theoretical modelling) available at the time from China – chart 7 in this piece being most relevant – https://medium.com/@tomaspueyo/coronavirus-act-today-or-people-will-die-f4d3d9cd99ca
which shows the time lag of discovered and reported cases to real existing unknown cases. The low numbers of official known UK cases in late February/early March will certainly have hidden a far greater number of cases of unknown cases not being contained and being spread through the “herd”. Even with the gerrymandered official figures on the low side its unsurprising that the UK has the worst mortality rate on the planet in terms of population. Its little wonder they stopped reporting the recovered/release figures side of the closed cases metric in mid-April with only a 3% survival rate in UK hospitals.
Financial assistance for those most impacted was and remains slow, bureaucratic and half hearted. At the same time public transport was drastically cut (for obvious health and safety reasons) which contributed to packed commuter transport and workplaces as some groups, construction workers among others, continued earning money desperately needed in an employment market context in which most people live from wage packet to wage packet.
Add to this the inadequate practical support in terms of PPE and similar equipment; amount of testing (the number of daily cases in the official data is dependent upon the limited number of tests carried out and in no way reflects the actual number of cases); the deliberate emptying of hospitals into care homes to hide the true figures; and the crude propaganda techniques utilised to divert attention from this apparent ‘failing/inefficiency’ on the part of Government – from weekly clap fests for NHS and care staff (from many voters who voted in policies designed to destroy the NHS only a few months ago) to requisitioning wartime nostalgia. Even the Imperial College model, alleged to be the sole criteria upon which decision making was based, factored in only 50% of the populace adhering to any kind of strict lockdown.
And despite the obvious high profile cases of police over zealousness featured on SM (which has existed and featured for years prior to this) most cases of ‘breaching’ the supposed draconian lockdown go unnoticed. (If there was a reward system for reporting them I could have been far from alone in being richer than Creosote by now).
The Government has certainly been inefficient and ineffective in every regard and the result of that inefficiency and ineffectiveness, with many associated failings including the current premature easing of restrictions, has a practical outcome congruent with the initial political decision to pursue a culling policy. Publicly “blaming” ‘The Science’ whilst not putting in place adequate systems to effectively and practically support the apparent change in policy has everyone arguing about “The Science” rather than focusing on the actual outcomes and politically based decisions which have been the actual driver of policy making decisions.
Much like the three cups and pea game which is also all about distraction.
Which from the perspective of those lining up the NHS and its assets for some pet projects – see here:
https://bylinetimes.com/2020/05/20/dominic-cummings-billion-dollar-brainchild/
and here:
https://bylinetimes.com/2020/05/14/whitehall-analytica-the-ai-superstate-part-2-is-covid-19-fast-tracking-a-eugenics-inspired-genomics-programme-in-the-nhs/
is a result. The valuable NHS assets have been secured (so far it has not been overwhelmed and fallen over); the apparent ineptness and inefficiency of this Government has spread the virus more thoroughly through the herd in line with the original culling rtequirements; and everyone is focusing on “The Science” as being the reason for decisions rather than the politics.
Yes, Johnson was basically coerced into locking down by Macron’s threat to close the borders, but this post isn’t about the decision to lock down: it’s about the earlier decision to abandon the original test-and-track strategy.
I would like a source for that 3% number. Also I don’t understand this:
The valuable NHS assets have been secured
Buildings and land don’t disappear because the queue outside gets really big. If you somehow travelled to Bergamo or Wuhan, where the system was overwhelmed, you’d find they’re all still standing. The point was that they were unable to care for patients through sheer volume of traffic.
This worldometer coronavirus data site provides daily data by country.
Clicking on many (but not all) country data will include up to date officially released data from the Government of that country for today of the closed cases metric. This metric splits into two parts;
1. The number of Covid-19 cases Released/Recovered (which leads to the reasonable assumption this is based on hospitalised cases only).
As an aside the data released out of China in the link to the Medium article by Tomas Pueyo suggested just under 81% of cases from China did not require any hospital intervention (these being ‘mild’ cases); around 13% required hospital treatment; whilst 4.7% needed critical care. It would seem reasonable to surmise that a lot of models from around the world at that time for the planning of likely hospital and CCB requirements would have used those figures.
2. The number of Covid-19 cases who died (again, to be consistent with the ‘Released’ side of the metric it is reasonable to assume this also is likely to be cases admitted to hospital).
I did not commence a daily spreadsheet log sample (of twenty countries) on this metric until discovering this site on 29 March.
On that date the number of cases recovered/released in the UK officially released figures was 10% (rounded) of the total number of closed cases for that day. That total number being the sum of both figures – number recovered/released and number of deaths on the day. The number of deaths being 90% (rounded) of the total closed case daily official figure.
From that point (29 March) the percentage figure of UK recovered/released (rounded) further reduced over a period of around 10-12 days down to less than 1% before rallying up to 3% (rounded) in the two or three days prior to April 13 when the UK Government figure for the recovered/released side of the metric stopped appearing.
This can be confirmed by clicking on the UK in the listed chart on the above link where the letters N/A appear in that side of that specific metric. As far as I can ascertain the only other Country of the list which has done the same thing (a few days after the UK) has been the Netherlands.
Whilst the Netherlands equivalent data was initially as poor as the UK’s it did get into double figures for a while before settling down to around 6-8% (rounded) before following the UK down the route of not releasing that figure. However, the official daily mortality case figure for the Netherlands was and remains a fraction of the equivalent UK official (hospital based) figure.
However, to be blunt:
A. I’m not convinced that meaningful international comparisons can be adequately made with the available official data, on at least this metric, for a number of reasons.
(i) I’m not confident that they are all collated using the same methodology. Some countriies only update the recovered numbers of a weekly basis whilst still releasing the mortality numbers daily (Republic of Ireland, on a Wednesday). Others (Germany) release recovered numbers which are consistently (as in every bleedin’ day) too neat – ie always exactly to the nearest hundred. Some suddenly post a massive increase in recovered cases they have seemingly just discovered which improves their recovery/mortality percentage ratio (Portugal, RoI). Others suddenly have an apparent change of collection methodology by posting aggragate figures from one or other side of this metric which are less than the previous day (China, Spain).
(ii) I am not confident in the efficacy of some of the official posted figures as they seem too good to be true (Brazil) or too low in aggregate terms for the size of population and observed infrastructure (India).
B. The UK official figures are a joke.
(i) On the closed cases metric recovered/recorded data only two sets of figures were ever released from the date I started recording that metric – ie the same figure was posted for a number of days every day and only increased slightly on one occassion and that remained the same until they stopped posting that figure on April 13.
It was such a low figure the only reasonable explanations I can conceive of is the UK Government (Johnson at al) don’t give a shit about that figure; can’t be bothered to collect that side of the data; it’s too embarrassingly low to officially release; or all three.
(ii) With the available real experience data from China showing a likely top figure to beat (ie achieve a lower percentage) of 4.7% of cases requiring critical care facilities it’s reasonable to anticipate the daily figure of UK critical care cases fluctuating – even if it is achieving a lower rate than the Chinese did.
What you don’t expect is the same unchanged figure for several weeks with only one change (an increase to 1559) which has stayed exactly the same for the best part of seven or eight weeks.
(iii) Even the daily figures cannot be relied on. It’s not quantum mechanics to add the daily figure of official cases to the previous day’s aggregate case figures to get today’s aggregate figure.
However, they have now managed to get that wrong on three occasions – in which the daily aggregate figure did not match the addition of the daily cases when added to the aggregate number of cases from the previous day (in each case a reduction/under recorded in the aggregate daily figure.
On the the two previous occasions I sent off an an email alert to the error – assuming I would not be the only saddo who noticed this and acted on it. Although never receiving a reply (other than the usual automated one) the aggravate figure was corrected within a day or two.
However, the most recent occurrence, about five days ago, I couldn’t be arsed. As of yesterday’s figures they are still repeating the original adding error and under-recording.
What would seem sensible to assume is that any politician or Government mindful of communicating it’s competence to the voting public at large in this scenario would be wanting to highlight successes. Everyone is fixated on the dire mortality numbers but no one seems to be balancing that with the numbers recovered. That this is not happening suggests, as observed above, that the figure is either too low or not being properly collected and collated.
Similarly with the critical care number.
Which neatly brings us to the second observation.
From my subjective way of thinking me and thee are of one mind on the fixed concrete NHS assets matter.
However, apart from becoming more cynical with age and everyday experience/observation, I’m mindful that oxygen breathers/movers and shakers (apply whatever label suits) seem to set a great deal of store by, and put a great deal of stock in, what appear to be labelled “intagible” assets.
Like confidence (public and private); organisational morale; performance indicators and probably a whole lot of similar intangibles others are more qualified than I to recognise and identify.
Overwhelming the NHS capacity leading to headline stories of people turned away for normal treatment in droves because the organisation has been under resourced in numerous ways over recent times to the extent that capacity cannot cope and there are no beds left; leading to even lower asset (staff) morale does not look good as a selling point to potential money making investors for the carpetbaggers currently pretending to Govern.
Far better to stifle public demand; shunt people with the virus back into the community and care homes; have new Nightingale hospital capacity unused with empty beds; and gerrymander and ignore inconvenient figures whilst at the same time giving off the well tried and tested Johnson air of incompetence in certain areas (poor PPE provison, unclear communications, slow and indecisive decision making etc).
He has a majority of 80. Tory MP’s are apparently being emailed to support the latest apparent (from Johnson at al’s POV) public debacle on the grounds they owe their seat to Cummings. The Opposition is now back to being the Loyal Opposition. The well tried and tested bread and circuses continues apace. SM local forums in the former ‘red wall’ areas continues to overflow with support for these charletans regardless.
Despite the current hiccup over Cummings the distractions and the smoke and mirrors which are the hall marks of Johnson’s career seem to be working.
Those of us appalled by this need to stop underestimating the way he operates via a vis his public persona act, up our game, and start thinking outside of what we thought was normal. Because that normal is unlikely to be coming back.
In the British Medical Journal of 23rd May 2020 (page 253) there is an article asking this very question. Apparently the House of Commons’ Science and Technology Committee sent a 19 page letter to the Prime Mininster after Public Health England failed to produce the evidence on which this decision was based. It is undoubtedly a key question though linked to plenty of other strange decisions.
Was a working strategy abandoned? That depends on whether preparations had been made to rapidly scale-up the testing, tracing and actions with people who had been traced. Possibly no preparations had been made, in which case the question is “Why not?” It should have been obvious this scale-up might be needed, and local authority staff had been waiting for the call to do contact-tracing for some time. Contact-tracing is an important part of understanding There may have been a panic when it was realised that scaling-up should have been prepared several weeks before (leading to test and trace being completely abandoned) but it doesn’t answer why Johnson’s government got to that stage.
If there is a earthquake in Mexico, everybody knows what they have to do. If there is a hurricane warning in Yucutan or in Cuba, or if strong winds or a volcanic eruption are forecast in Iceland, everybody knows what to do. There is a plan that has been rehearsed and refined, and it is followed because time is important and there is little time for debate. The debates were held when the plan was developed not when the emergency has arrived.
A pandemic was the number one security risk for the UK, and there was in theory a plan, so it is very odd that there are debates about strategy in the middle of an emergency.
In the Wikipedia article about Operation Cygnus, it says “According to the Telegraph, the exercise led to assumptions that a “herd immunity” approach would be the best response to a similar epidemic.” That means that somebody decided that the scale of preparations that would be required for a pandemic would be so great that somebody in government decided that the government wouldn’t bother making preparations. I don’t know whether that is true, but I can imagine certain members of the present-day Conservative Party having difficulty in getting their head around the responsibilities of a Government for these kinds of emergencies (as we have discussed before with respect to Cameron and flooding).
Permalink